Author: Dr H. Hunter Handsfield Clinical Professor of Medicine University of Washington 2008-10-20
 |
| Treponema pallidum bacteria. Source CDC |
Syphilis is one of the five originally recognized venereal diseases, with gonorrhea and the now rare sexually transmitted diseases (STDs) chancroid, lymphogranuloma venereum, and Donovanosis (granuloma inguinale). The causative organism, which belongs to a class of bacteria called spirochetes, is Treponema pallidum, one of the few important disease-causing organisms that still has not been successfully grown in the laboratory, significantly affecting diagnosis and impeding research.
This article addresses syphilis in the United States. The information on
frequency, risk factors, and populations at risk apply generally to
other industrialized countries; the descriptions of symptoms,
complications, treatment, and prevention are applicable everywhere.
HISTORY
It
is difficult to overstate the significance of syphilis and its impact
on human history and culture. It was long believed that syphilis was
introduced to Europe by crewmembers of Columbus’ expeditions who were
infected in the Americas. However, other syphilis-like infections
caused by closely related spirochetes—including the modern diseases
called yaws, pinta, “endemic syphilis,” and perhaps other now-extinct
variations of the disease—probably evolved in most human populations,
and the “Columbian” theory remains uncertain, despite the recent
exploitation of modern methods to analyze the genetic relatedness of
various strains of T. pallidum and other spirochetes. Whatever its
origins, the European syphilis epidemic of the late 15th and early 16th
centuries, spreading northward from what is now Italy, clearly was new.
Controversy exists as to whether morbus gallicus (the French disease),
the dominant name at the time, was more severe or death rates higher
than experienced in later centuries. Rapid spread in a previously
unexposed population could enhance the frequency of severe outcomes, but
it is equally plausible that early writers unwittingly (or perhaps
intentionally) exaggerated their descriptions of a new condition
attributed both to a foreign invader and divine retribution.
The
social and cultural echoes of syphilis reverberate today. Syphilis was
“the pox,” with innumerable references throughout the works of
Shakespeare. Later it became known as “the great pox” to contrast with
“the small pox,” which had its own historical impact. Many historical
personages were infected, apparently including Henry VIII and Beethoven,
in whom it is thought by some historians to explain the former’s
megalomania and the latter’s deafness. Nietzsche’s “Man and Superman”
probably was influenced by the author’s syphilitic dementia, and that
work is said to have influenced Hitler, himself believed to have been
infected most of his life. Ibsen’s play “Ghosts” is a story of
syphilis, as is Leroux’s “The Phantom of the Opera,” although that
aspect was not explicit in the Andrew Lloyd Webber version. The Latin
word for syphilis, lues, led to unsavory literary characters named Louie
by Hemingway and other authors. Spencer Churchill’s mental illness,
abandonment of family, and early death were attributed to syphilis and
may have influenced his son Winston’s incomparable drive to excel. The
mid-twentieth century Tuskegee study of untreated syphilis, in which the
United States Public Health Service withheld treatment from poor
African American men for three decades, even after penicillin became
available, stands as a signal event both in modern race relations and
international policies on research in human subjects.
HOW COMMON IS SYPHILIS AND WHO IS AT RISK?
Frequency
Unlike
most STDs, of which many cases go undiagnosed and unreported, almost
all diagnosed cases of syphilis are confirmed by laboratory testing, and
almost all laboratories routinely report their positive syphilis test
results to local or state health departments. Therefore, the data are
more complete than for most reportable conditions, so that official case
rates are highly accurate. Accurate statistics are lacking outside
industrialized countries.
How Trends are Measured.
Syphilis is categorized into stages, described in detail below.
Primary syphilis is usually apparent 2-6 weeks after exposure and the
secondary stage usually occurs 2-4 months later. Following the
secondary stage, the infection becomes asymptomatic, or latent, further
divided into early latent (under a year in duration) and late latent
cases (a year or more since infection). The true total of new
infections each year is close to the sum of primary, secondary, and
early latent cases. For example, in 2006 there were 9,756 reported
cases of primary and secondary syphilis and 9,186 cases of early latent
infection, for a total of 18,942 cases. However, it can be difficult to
distinguish early latent and late latent syphilis. Therefore, to
maximize transmission, the total of primary plus secondary syphilis
cases is generally used for year-to-year comparisons and to track rates
over time.
Rates of Primary and Secondary Syphilis.
This graph shows the reported rates of primary and secondary syphilis
per 100,000 population since 1987, with separate lines for trends in men
and women. Two salient observations are apparent. First, as shown in
the solid line, the count rose to a peak of 20.3 cases per 100,000 in
1990, the highest rate since 1949; declined ten-fold to case rates of
2.1 in 2000 and 2001; then began to rise. Although the slope of the
line does not look alarming, the rate of 3.3 cases per 100,000 in 2006
represents a dramatic 57% rise since 2001.
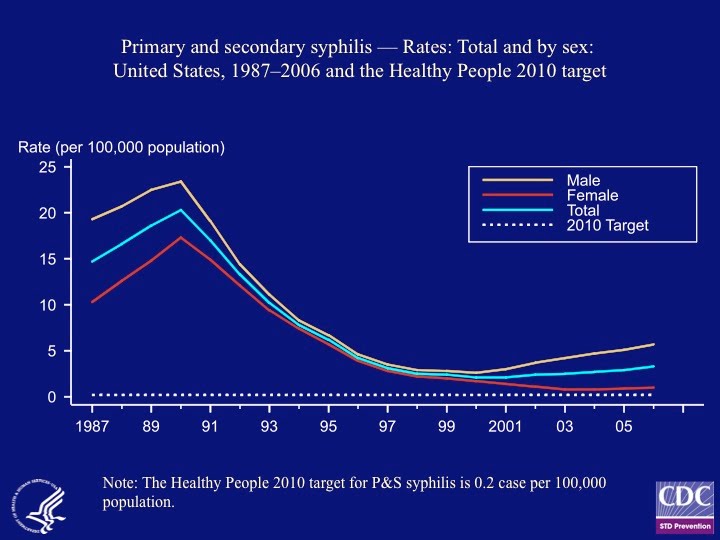
Second,
for many years the rates in males and females converged on one
another. In 1987 the rate in men was double that in women, about 20 and
10 cases per 100,000, respectively. By 1998, the case rates in men and
women were ten-fold lower and nearly equal. Since then the male and
female case rates have diverged once again, so that in 2006 the rate was
almost 6 times higher in men than in women. These observations are
explained by opposite trends in syphilis control among heterosexual men
and women compared with men who have sex with men (MSM). As the
incidence of syphilis rose in the late 1980s, most cases occurred in
heterosexuals, driven by high rates of substance abuse (especially use
of crack cocaine) in inner city environments, in concert with
drug-related commercial sex. At the same time, cases in MSM began to
decline rapidly because of behavioral changes in response to the
emerging AIDS epidemic. The divergent male and female case rates in the
past several years reflects both rising rates in MSM, resulting from a
let-down in safe sex practices in response to improved HIV treatment and
survival, and continuing improvement in syphilis control in
heterosexual men and women.

Trends in Congenital Syphilis.
Congenital syphilis of newborns results from transmission of infection
from mother to fetus, and the rates parallel those in women. Three
hundred forty-nine cases were reported in 2006, a rate of 8.5 per
100,000 live births. Reported rates somewhat underestimate the actual
disease burden, because some congenital infections result in miscarriage
or premature stillbirth without diagnosis. Nonetheless, the rate
declined from 651 per 100,000 births in 1941, a 76-fold difference, one
of the great achievements of public health. Today most cases of
congenital syphilis occur in highly disadvantaged populations, in
infants born to mothers who do not receive prenatal care, especially in
immigrant Hispanic populations. Many cases are directly attributable to
policies that dissuade undocumented immigrants from accessing health
care.
Populations with Syphilis.
In 1999, the US Centers for Disease Control and Prevention (CDC)
announced the national plan to eliminate syphilis transmission in the
United States. From the perspective of prevention experts viewing the
trends in the 1990s, that goal seemed realistic. The syphilis
elimination plan brought considerable benefit in controlling
heterosexually transmitted syphilis, including virtual elimination of
the disease from some metropolitan areas. Nevertheless, for the
foreseeable future elimination is a forlorn hope. Still, syphilis now
is a highly focal disease, and relatively few sexually active persons
are at significant risk. About two-thirds of cases occur in MSM, and
heterosexually transmitted cases are concentrated in a few particularly
disadvantaged populations, such as poor minorities in inner cities and
southeastern states, and immigrant populations in the Southwest.
As
for all STDs, race and ethnicity also are associated with syphilis, a
reflection of socioeconomic status, access to health care, and
differences in sex partner networks (but not to promiscuity, since the
average number of sex partners does not vary significantly by race).
Compared with whites, in 2006 the rates of primary and secondary
syphilis were six-fold higher in blacks, and twice as high in Native
Americans and persons of Hispanic ancestry. The lowest rate occurs in
persons of Asian or Pacific Island ancestry.

Syphilis
is closely linked with human immunodeficiency virus (HIV) infection and
AIDS, especially among MSM. A minority of MSM remain highly sexually
active and inconsistently follow safe sex guidelines, comprising the
core population for both syphilis and new HIV infections in the United
States and most industrialized countries. For example, about 60% of
people with primary or secondary syphilis in King County, Washington are
HIV positive. As shown in this figure, the estimated rate of early
syphilis in MSM in King County rose from nil in 1997 to almost 2,000
cases per 100,000 HIV infected MSM in 2005 (i.e., almost 2% of
HIV-infected MSM acquire syphilis each year), and to a rate of almost
200 in HIV negative MSM. These rates are roughly 500-fold and 50-fold
higher, respectively, than the overall rate of early syphilis in the
United States, and are among the highest rate of syphilis ever
documented in any population. Although such analyses have not been done
elsewhere, it is likely that the rates are similar in other cities, and
probably one third to half of all new syphilis infections in the United
States occur in HIV-infected persons. (Figure from Kerani et al 2007;
see Suggested Reading.)
Transmission
Aside
from congenital transmission to unborn children, syphilis is
transmitted primarily by sexual activity. However, syphilis carries a
greater potential than most STDs for nonsexual transmission. In the
pre-antibiotic era, there were relatively frequent reports of
transmission by blood transfusion, wet nurses infected by babies with
congenital syphilis, dentists and physicians who sustained infections of
the fingers in the course of caring for infected patients, and
presumably “innocent” transmission among children in orphanages. (The
last might now be questioned in light of modern knowledge of child
sexual abuse).
As
for all sexually transmitted organisms, the syphilis spirochete does
not survive drying or other environmental stresses, so that transmission
requires the direct exchange of infected secretions or apposition of
moist, infected surfaces, conditions that in adults are almost entirely
limited to sex. Insertive penile-vaginal and penile-anal intercourse
are the dominant practices that transmit syphilis, although oral-genital
and oral-anal contact account for a substantial minority of cases.
Transmission by kissing is theoretically possible but rarely if ever
documented. Sexual transmission a year or more after infection is rare,
except that congenital transmission can occur during all stages of
syphilis.
WHAT ARE THE SYMPTOMS AND SIGNS OF SYPHILIS?
The
manifestations of syphilis are very broad, with the potential to mimic
many other medical conditions. The disease has been characterized as
“the great imitator”, a characteristic also reflected in repeated,
oft-quoted statements by Sir William Osler, the father of modern
medicine, which approximate “He who knows syphilis, knows medicine.”
The descriptions that follow are common and often classical, but
atypical cases abound; comprehensive descriptions literally have filled
entire textbooks.
Primary Syphilis
 The hallmark of primary syphilis is the chancre, an open sore at the site where T. pallidum
is inoculated. The chancre usually appears 2 weeks to 6 weeks after
exposure, starting as a papule, i.e., a bump on the skin, that soon
ulcerates. The most common sites are those most subject to sexual
friction, because infection usually occurs where the spirochete is
massaged into exposed tissues, perhaps aided by microscopic trauma.
Accordingly, chancres most commonly occur on the penis, especially on
the glans (head); the labia or at the vaginal opening; the anus,
especially in MSM; and sometimes the lips or tongue.
The hallmark of primary syphilis is the chancre, an open sore at the site where T. pallidum
is inoculated. The chancre usually appears 2 weeks to 6 weeks after
exposure, starting as a papule, i.e., a bump on the skin, that soon
ulcerates. The most common sites are those most subject to sexual
friction, because infection usually occurs where the spirochete is
massaged into exposed tissues, perhaps aided by microscopic trauma.
Accordingly, chancres most commonly occur on the penis, especially on
the glans (head); the labia or at the vaginal opening; the anus,
especially in MSM; and sometimes the lips or tongue.
The
typical chancre is a single lesion, painless or with only mild
discomfort. Swelling of the immediately adjacent tissues results in a
firm, rubbery consistency that helps distinguish syphilis from herpes
and other causes of genital ulcer disease. The photographs shows two
typical examples, except that dual lesions are uncommon. However,
atypical lesions are common and include multiple or painful lesions,
occurrence at nongenital sites of exposure, and internal lesions
(vagina, cervix, rectum) that the patient may not notice. Nearby lymph
nodes often are enlarged, especially in the groin or, for oral lesions,
under the jaw or in the neck. All these symptoms commonly are absent,
because the chancre itself can be small, transient, or internal, and
subtle lymph node enlargement may not be noticed. Therefore, probably
about one third of patients with primary syphilis are asymptomatic.
Systemic symptoms, such as fever, are absent. Without treatment, the
chancre heals and enlarged lymph nodes regress, typically over 2-6
weeks.
Secondary Syphilis

During
the primary stage, the spirochete enters the bloodstream and
disseminates throughout the body, without symptoms, setting the stage
for secondary syphilis. The most common manifestation of secondary
syphilis is a skin rash. The classical appearance is termed
“papulosquamous,” i.e. the dominant features are papules (slightly
raised bumps and patches) that often are accompanied by flaking of
superficial (squamous) layers of the skin. Itching usually is absent.
Any part of the body may be affected, but the trunk and limbs are most
commonly involved. A classical feature is involvement of the palms and
soles, which is infrequent in most other skin rashes; sometimes the
occurrence of a rash on the palms or soles is the clinician’s first clue
to secondary syphilis. Patchy hair loss can occur when the scalp is
affected. In moist areas of the body, such as the genital area, near
the anus, and in the mouth, the rash of syphilis can cause flat,
painless lesions called mucous patches, ulcerating lesions, or warty
lesions called condylomata acuminata. Such moist lesions of secondary
syphilis are teeming with spirochetes, and transmission of syphilis to
sex partners probably is most frequent during the secondary stage.

Syphilitic
rashes are highly variable and can mimic numerous other common skin
conditions, including psoriasis, certain fungal infections such as
lichen planus, allergic drug rashes, patchy loss of pigment (vitiligo),
and numerous others. Perhaps the single most frequent error in
diagnosing syphilis is the failure of clinicians to request syphilis
blood tests in patients with unexplained rash.
Secondary
syphilis is more than a rash, and any organ may be affected. Lymph
nodes may enlarge in several areas of the body. Fever is common,
although often it is mild and may go unnoticed by the patient. The
liver or spleen may enlarge. The eyes can be affected, with
inflammation of the iris, retina, and surrounding structures (uveitis),
and kidney disease and arthritis sometimes occur. Headache, hearing
loss, and other manifestations of infection of the central nervous
system also are common, as discussed below (Neurosyphilis).
Like
primary syphilis, the secondary stage resolves spontaneously, usually
over 1-3 months, as the immune system brings the infection under partial
control. However, spirochetes survive inside the cells of most if not
all organs. Secondary syphilis sometimes recurs up to a year, and
rarely up to four years, after the initial infection.
Latent Syphilis
By
definition, syphilis is latent when infection persists in the absence
of outward manifestations and can be detected only by laboratory
testing. Early latent syphilis refers to infection up to one year in
duration, whereas more prolonged asymptomatic infection is called late
latent. Many persons with early latent syphilis remain infectious
through subtle, unrecognized lesions, such as mucous patches in the
mouth, vagina, or rectum. On careful examination, some asymptomatic
persons with apparent early latent syphilis in fact have continuing mild
manifestations of secondary syphilis. Late latent syphilis can no
longer be transmitted, except to fetus in pregnant women.
Tertiary Syphilis
The
tertiary stage of syphilis can appear any time after a year. Most
cases occur within 30 years, but the potential for reactivation
continues for life. The spirochetes that seed most organs during
primary and secondary syphilis typically remain inactive, held in check
by the immune system. However, if immune control fails, latent
organisms can reactivate. Sometimes this occurs when cancer, AIDS, or
other disease impairs immunity, but usually no obvious explanation is
apparent. The result is tertiary syphilis, characterized by localized
tissue destruction.
Three types of tertiary syphilis once were common. Cardiovascular syphilis results from infection of the aorta, causing secondary damage to the heart. Gummatous
syphilis is characterized by the gumma, a tumor-like lesion so named
from the Latin for its rubbery consistency. Gummas usually involve the
skin, bones, and joints, but any organ may be affected, with
irreversible damage caused by tumor-like growth. Third, tertiary neurosyphilis
causes a number of central nervous system manifestations, including
stroke, blindness, deafness, paralysis and, most important from a
historical perspective, “general paresis of the insane,” once the
dominant cause of dementia worldwide and the explanation for much of the
social impact of syphilis for five centuries. All forms of tertiary
syphilis now are rare in industrialized countries, the result of
improved diagnosis of latent infection and the development of effective
treatment. In addition, many persons undergo antibiotic therapy for
various conditions, unknowingly being treated for undiagnosed latent
syphilis.
Neurosyphilis
Commonly
considered a manifestation of tertiary syphilis, neurological
involvement actually is most frequent during the early stages, within a
year of infection. Tertiary neurosyphilis now is a medical curiosity in
industrialized countries, while awareness of early neurosyphilis is on
the rise. The central nervous system is inoculated when spirochetes
circulate in the blood, and T. pallidum often can be found in the
cerebrospinal fluid of persons with primary or secondary syphilis but
no apparent neurological problem. In those with symptoms of early
neurosyphilis, the main manifestations are headache, hearing loss,
blindness, and stroke, potentially devastating complications in
otherwise healthy young persons. All of these appear to be more common
in HIV infected persons, who comprise up to half of all persons with
early syphilis in the United States. Fortunately, routine treatment for
primary, secondary, or early latent syphilis probably eradicates most
infections of the central nervous system. However, diagnosis of
neurosyphilis requires spinal tap in order to test cerebrospinal fluid,
engendering controversy about how aggressively asymptomatic
neurosyphilis should be sought and whether more aggressive treatment
lowers the risk of serious outcomes.
Congenital Syphilis
Once
common worldwide and now rare in industrialized countries, congenital
syphilis continues to be a major cause of stillbirth and lifelong
disability in developing countries. In infected babies who survive to
birth, the most severe form of congenital syphilis is a devastating
systemic infection, in essence an aggressive form of secondary syphilis
with multiple organ failure, often resulting in early death or
neurological damage in survivors. Survivors of milder infection suffer
such complications as abnormal bone growth leading to facial and other
deformities, dental malformation, hearing loss, and psychological
disabilities. Other congenital infections are entirely asymptomatic, detected only by laboratory testing.
HOW IS SYPHILIS DIAGNOSED?
Syphilis
can be suspected by the trained clinician based on symptoms and
physical examination and further informed by the epidemiological
context, such as the gender of sex partners or other indicators of
higher risk. However, laboratory diagnosis is essential in all cases.
Identification of Treponema pallidum
Unlike
the organisms that cause most STDs, the syphilis spirochete cannot be
cultured and DNA detection tests are available only in a few research
laboratories. Even the simple technique of staining specimens to
identify the organism microscopically is not practical to identify T. pallidum.
The organism can be visualized by specialized “dark field” microscopy,
taking advantage of the characteristic shape and motility of the
organism, [Figure] but this cumbersome technique requires immediate
examination of scrapings of chancres or skin lesions while still moist,
and is rarely available outside health department STD clinics. These limitations have serious implications for diagnosis .
Blood Tests
Except
for primary and some cases of secondary syphilis, serology—testing of
blood to detect antibody, the immune system’s reaction to syphilis—is
the mainstay of diagnosis, and the only means of diagnosing latent
infection and most cases of neurosyphilis or tertiary disease.
The
Wasserman test, developed near the turn of the twentieth century, was a
critical advance in its day. Essentially the same test persists today
in the form of the “nontreponemal” blood tests. The most common of
these are the test developed by the Venereal Disease Research
Laboratory, the forerunner of today’s CDC, and therefore known as the
VDRL test; and the rapid plasma regain test, or RPR. Both tests are
highly sensitive, missing few if any active cases of syphilis, once
enough time has passed (4-6 weeks) for the tests to become positive.
However, both the VDRL and RPR are nonspecific, meaning they are prone
to give false positive results in persons without syphilis.
Therefore,
positive VDRL or RPR tests are always confirmed by testing the same
blood specimen with a “treponemal” antibody test that measures antibody
to T. pallidum itself. For several decades, the dominant
treponemal test was the fluorescent treponemal antibody-absorbed test,
or FTA-ABS. Like the VDRL, The FTA-ABS was developed at CDC and was
made available worldwide at no cost. The FTA-ABS remains in use in
special circumstances, but the most widely used treponemal test now is
the Treponema pallidum particle agglutination test, or TPPA.
In
the United States, most syphilis testing is initiated with RPR or VDRL,
and positive results are confirmed by TPPA. With rare exceptions,
positive results on both tests is definitive evidence of syphilis. The
strength of the VDRL or RPR result is related to the duration and
activity of infection, with maximum strength typically during secondary
syphilis, the strength of the positive result declines after effective
treatment. Therefore, the RPR or VDRL result gives clues about the
likelihood of primary, secondary, or other stages of infection, and the
decline after penicillin therapy helps measure the effectiveness of
treatment. Serological tests also are done on cerebrospinal fluid to
diagnose neurosyphilis.
A
recent advance in syphilis serology is the development of automated
treponemal antibody tests that can be done more rapidly and more cheaply
than RPR or VDRL, including fast, simple tests done on a drop of blood
obtained by finger prick that can be performed with minimal equipment in
resource-poor settings. Taking advantage of these technologies,
initial testing increasingly is done in the opposite sequence than in
the past, i.e. a rapid treponemal test followed by RPR or VDRL on
positive specimens.
Although
laboratory testing is crucial, accurate diagnosis of syphilis often is
highly dependent on the clinical judgment of well trained and
experienced clinicians. With all test methods, it often takes 4-6 weeks
after infection the tests to become positive. Therefore, some recently
exposed patients are infected yet have negative results. In patients
with chancres indicating newly acquired primary syphilis, up to 40% have
negative blood tests. Finally, both false negative and false positive
test results occur in other clinical settings. Laboratory confirmation
of neurosyphilis frequently is especially difficult.
HOW IS SYPHILIS TREATED?
Syphilis
is nearly unique among human diseases, by virtue of the fact that
penicillin remains the drug of choice and is still the most reliable
form of treatment more than six decades after the drug came into use.
In addition, T. pallidum is one of a very few pathogenic bacteria
that have not developed significant resistance to antibiotics, with the
single exception of recent evolution of some strains resistant to the
drug class called macrolides (erythromycin, azithromycin, and related
drugs). Penicillin remains the drug of choice for all stages of
syphilis, even in patients who previously experienced allergic reactions
to the drug. When strong reasons preclude penicillin therapy, the
tetracycline class of drugs, such as doxycycline (Vibramycin® and
generic brands) and the cephalosporins, such as ceftriaxone (Rocephin®),
can be used. Many other antibiotic classes are entirely inactive
against syphilis and have no role in treatment, including the
sulfonamides (“sulfa” drugs), aminoglycosides like streptomycin and
related drugs, and the fluoroquinolones, such as ciprofloxacin (Cipro®).
The table below lists the main treatment regimens recommended by CDC http://www.cdc.gov/std/treatment/2006/toc.htm.
For early syphilis, a single intramuscular injection of benzathine
penicillin, a “repository” version of the drug that is absorbed into the
bloodstream from the injection site over 1-2 weeks, immediately aborts
infectivity and usually is curative. Three doses of benzathine
penicillin at weekly intervals are recommended for syphilis more than a
year in duration. High dose intravenous penicillin is used for
symptomatic neurosyphilis and congenital syphilis.
Treatment of Syphilis
Primary, Secondary, and Early Latent Syphilis
Benzathine penicillin G, 2.4 million units by intramuscular injection
Late Latent Syphilis and Tertiary Syphilis (Except Neurosyphilis)
Benzathine penicillin G, 2.4 million units by intramuscular
injection, 3 doses at weekly
intervals
Neurosyphilis
Aqueous penicillin G, 18-24 million units intravenously per day, in
divided doses or by continuous
infusion, for 10-14 days
OR
Procaine penicillin G, 2.4 million units by
intramuscular injection once daily, PLUS
probenecid, 500 milligrams 4 times daily, for 10-14 days
Treatment
generally is given before diagnostic confirmation in order to
immediately prevent disease progression and complications and to prevent
transmission by those who might continue to place their sex partners at
risk. The sex partners of persons with infectious syphilis are treated
regardless of whether or not they are found to be infected, in order to
abort incubating infection. Similarly, babies born to infected mothers
are treated without waiting for evidence that they actually are
infected.
Documenting
that treatment is effective can be a challenge. In most successfully
treated patients, the RPR or VDRL becomes negative, or at least the
strength of the positive test result declines dramatically. But
sometimes the test result changes little, leaving the outcome in doubt.
In a few cases, overt treatment failure occurs, especially when drugs
other than penicillin are used, and rarely after penicillin treatment
itself. Treatment failure usually is manifested only by return of the
blood test to positive, or strengthening of a weakly positive result, so
that persons treated for syphilis often require prolonged follow-up,
sometimes for several years, for repeat blood tests.
HOW IS SYPHILIS PREVENTED AND CONTROLLED?
Prevention
and control of STD can be viewed from the perspective of the individual
at risk, who prefers to avoid infection or, if already infected, wants
to prevent complications; and from the perspective of health care
providers and prevention agencies, such as health departments. These
perspectives overlap with one another. For example, health care
providers are advised to routinely test patients at risk for gonorrhea,
but sexually active persons can request testing when the provider does
not take the initiative. Similarly, providers should promote condom
use, but only persons at risk can choose to use them. Prevention of all
STDs, including HIV, is comprehensively addressed in the Knol on safe
sex. [link]
In
the distant past, a common syphilis prevention strategy was quarantine,
and often incarceration, of infected persons or those considered to be
at risk, such as prostitutes and “loose women.” (It was almost always
women who were subjected to such strategies, or native populations in
colonial lands, despite the obvious truth that most syphilis and other
STDs were imported by the colonizers.) If not incarcerated, infected
persons were ostracized (“The Phantom of the Opera”). “Moral
prophylaxis” included public shaming of infected persons, laws that
attempted to enforce abstinence or sexual fidelity, religious
sermonizing, and intermittently draconian approaches to preventing
prostitution and, paradoxically, suppression of knowledge about and
access to condoms. Such methods invariably failed and pragmatism
eventually reigned; most of these strategies were attempted fitfully,
followed by return to the status quo.
Screening
populations with syphilis blood tests has been a mainstay of syphilis
prevention for a century. Because current tests are inexpensive, blood
screening often is cost effective even in persons at relatively low
risk, and testing to detect asymptomatic infection is routine in persons
obtaining care for other STDs, in MSM seeking routine health care, and
in other populations at high risk (e.g., jail and prison inmates).
Additionally, routine testing is done in most pregnant women as a
strategy to prevent congenital syphilis.
Other
key prevention strategies emphasize populations at particular risk, and
include promotion of condom use and other aspects of safe sex, symptom
awareness, treatment of infected persons, and notification and treatment
of exposed partners. However, all prevention strategies are challenged
by the current epidemiology of the disease. The syphilis epidemic in
the United States and most industrialized countries has “contracted”
around particularly high risk populations that typically are
socioeconomically disadvantaged, subject to prejudice, or have
especially high frequencies of anonymous partnerships, such as some MSM,
commercial sex workers and their partners, and undocumented
immigrants. Continued syphilis is largely determined by behavioral
patterns that include substance abuse, high rates of psychological
morbidity, anonymous partnerships, resistance to condom use, and often
reduced access to health care. Selective mass treatment, i.e.,
distribution of antibiotics to entire groups of persons at risk, has
been tried and found ineffective. Collectively, these difficulties
explain the futile hope, described above, for syphilis elimination.
SUGGESTED READING
1.
Sparling PF, et al. Clinical Manifestations of Syphilis. Chapter 37
in Holmes KK, et al (ed). Sexually Transmitted Diseases, 4th edition.
New York, McGraw-Hill, 2008:661-84. The main chapter in the premier STD textbook.
2.
Handsfield HH. Syphilis. Chapter 4 in Handsfield HH, Color Atlas and
Synopsis of Sexually Transmitted Diseases, 2nd edition. New York,
McGraw-Hill, 2001:33-54. An extensively illustrated review, intended for health professionals but easily understood by all readers.
3. CDC. Sexually Transmitted Disease Surveillance, 2006. Atlanta, GA, November 2007. http://www.cdc.gov/std/stats/trends2006.htm Annually updated statistics on reported STD in the United States.
4. CDC. Sexually Transmitted Diseases Treatment Guidelines, 2006. Morbidity and Mortality Weekly Report 2006;55:RR-11. http://www.cdc.gov/std/treatment/2006/toc.htm CDC's treatment recommendations, including summaries of key information about all STDs.
5. Kerani RP, et al. Rising rates of syphilis in the era of syphilis elimination. Sexually Transmitted Diseases 2007;34:162-5. Analysis of disease trends, with emphasis on resurgent syphilis and other STDs in men who have sex with men.
6. Marra CM. Déjà vu all over again: when to perform a lumbar puncture in HIV infected patients with syphilis. Sexually Transmitted Diseases 2007;34:145-6. An
editorial that reviews current controversies on the importance of early
recognition and diagnosis of neurosyphilis in the presence of HIV
infection.