Authors: Drs Tom F Lue and Alan Shindel University of California San Francisco 2008-11-12
Male Sexual Function and Dysfunction: A guide for men and their partners. This article is a review of normal sexual function in men. It also contains information on sexual problems that may affect a man at different points in his life. It is written for men and their sexual partners.
Normal male sexual functionMale Sexual Function and Dysfunction: A guide for men and their partners. This article is a review of normal sexual function in men. It also contains information on sexual problems that may affect a man at different points in his life. It is written for men and their sexual partners.
How does the penis become erect?
The human penis is composed of three cylinders of spongy tissue. There are two corpora cavernosa which are located on the top side of the penis. The third cylinder is called the corpus spongiosum. The
corpus spongiosum connects with the head (glans) of the penis, and the
urethra (water channel) runs through the corpus spongiosum.[1]
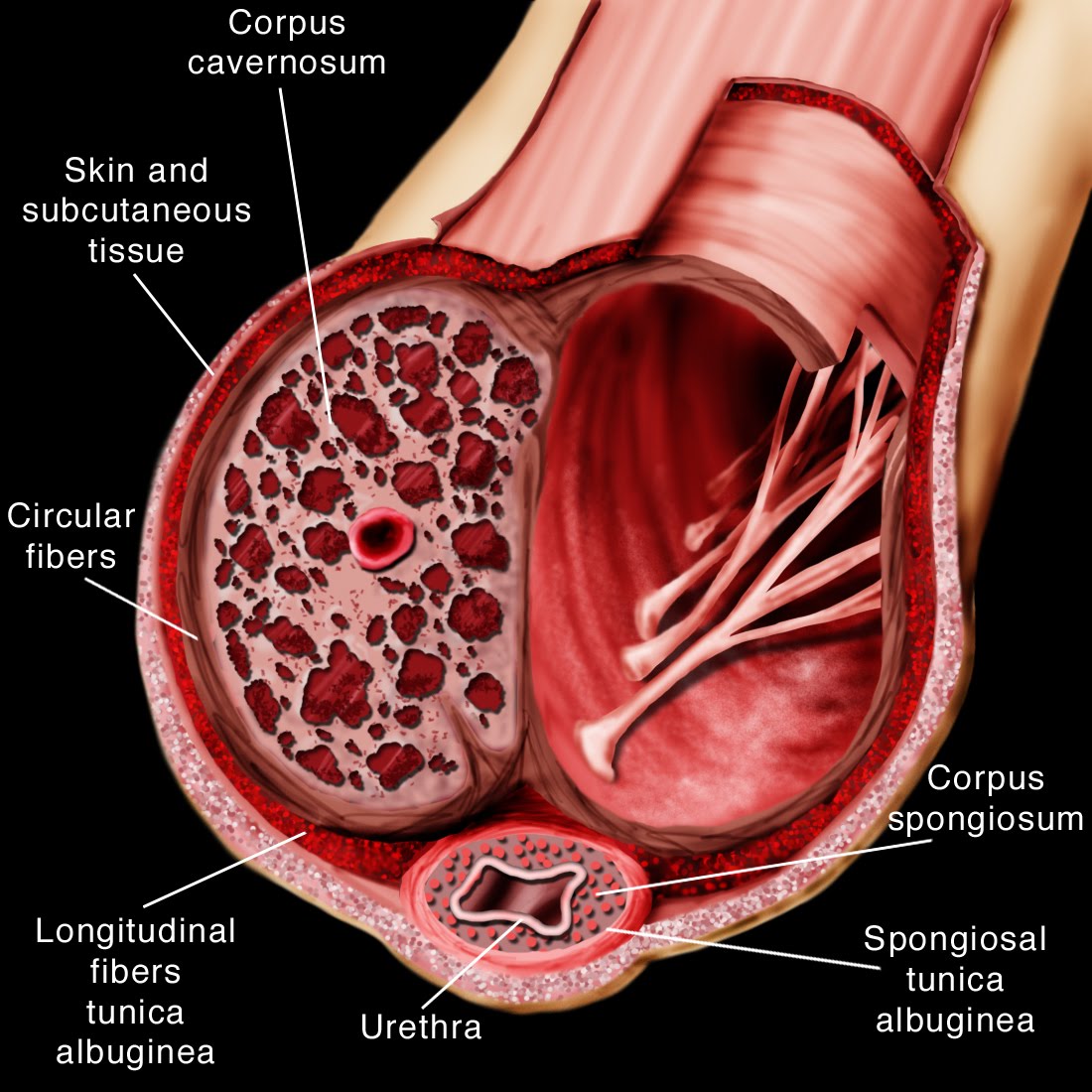
Image reproduced by William Haun (http://www.willhaun.com)
When a man is sexually stimulated, nerve signals are transmitted from the hypothalamus
(the part of the brain that integrates the things a man sees, hears,
smells, feels, and thinks) through the spinal cord to specialized nerves
in the sacral portion of the spinal cord, which is part of the parasympathetic nervous system.
The sacral spinal cord is connected to nerves in the pelvis which, when
stimulated, cause muscle relaxation in the walls of small arteries and
spongy tissue inside the corpora cavernosa of the penis. This relaxation is mediated through two important molecular messengers; nitric oxide (NO) and cyclic GMP (cGMP).[1]
The
process of muscular relaxation leads to dilation (opening) of these
blood vessels and an increase in blood flow to the spongy tissue of the
corpora cavernosa. This increase in blood flow causes enlargement of the corpora cavernosa and the penis. While
this is occurring, small veins that drain the corpora cavernosa are
compressed between the swelling spongy tissue and a tough layer of
tissue that surrounds the corpora (the tunica albuginea). Compression of these veins prevents blood from leaving the corpora cavernosa so that the penis swells full of blood. During this first phase of erection, the shaft of the penis becomes firm but the head of the penis may not be hard. As sexual excitement increases, contraction of the ischiocavernous and bulbospongiosus muscles
at the base of the penis forces more blood into the corpora cavernosa
and corpus spongiosum, which increases the rigidity of both the shaft
and head of the penis. This corresponds to the rigid, maximally engorged phase of penile erection. After intercourse or when the sexual stimulus is removed, this process reverses and the penis becomes flaccid again.[1]
How does ejaculation (coming) occur?
Ejaculation (expulsion of semen from the penis) and orgasm (an
intense sensation of pleasure with sexual climax) typically occur
together in men but represent distinct physiological events. This discussion will focus on ejaculation.
Ejaculation
is a complex process that involves tight coordination of the nervous,
muscular, and urogenital systems. Ejaculation itself is divided into two
distinct phases, emission and ejection. Both of these processes occur within a matter of seconds.[2]
What occurs during the emission phase?
During emission a number of events (depicted in the diagram below) occur in rapid succession. The muscular bladder neck and external urethral sphincter
tighten in the innermost portion of the urethra. Shortly thereafter,
fluid from the seminal vesicles and prostate (grey arrows) is deposited
in this portion of the urethra, where it mixes with sperm (white arrow)
that travel through a tube attached to the testicle called the vas deferens. This fluid and sperm mixture is known as semen.

Image reproduced by William Haun (http://www.willhaun.com)
What occurs during the ejection phase?
During
ejection (see diagram below) the external urethral sphincter opens up,
permitting semen to pass into the portion of the urethra beyond the
prostate. Strong contractions of the bulbospongiosus muscle (grey
arrows) then force the semen out of the urethral meatus (the hole at the
tip of the penis).

Image reproduced by William Haun (http://www.willhaun.com)
What role does the spinal cord play in ejaculation?
During
penile stimulation (from intercourse or masturbation), sensory
information from the penis is communicated to the lower portion of the
thoracic spinal cord, which is part of the sympathetic nervous system.
At some threshold level, the signal from the penis stimulates the
spinal cord to send a message to the lower urinary tract, which causes
emission of semen and contraction of the bladder opening (this keeps
semen from backing into the bladder).
Ejection occurs when sensory nerves in the urethra detect the presence of semen. These nerves transmit a signal to the sacral spinal cord, which in turn stimulates strong contractions of the bulbospongiosus muscles which surround the urethra. These contractions force the semen out of the body.
What role does the brain play in ejaculation?
In
humans, the brain sends signals that inhibit the ejaculatory centers of
the thoracic and sacral spinal cord under normal conditions. Because
the brain has control over the ejaculatory centers of the spine, most
men are able to exercise some degree of control over ejaculation. In
a process similar to what occurs in the spinal cord, at some threshold
level of sexual excitement, the inhibitory signal from the brain to the
spinal cord ejaculation center is “turned off” and ejaculation will
occur if adequate penile stimulation is also present.
While
the exact process by which the brain regulates ejaculation has yet to
be conclusively demonstrated, two neurotransmitters (chemicals used by
nerves to communicate with one another) appear to play central roles. Serotonin plays an inhibitory role (that is, delays ejaculation) and dopamine
plays a stimulatory role (that is, speeds ejaculation). Use of
medications that modulate serotonin and dopamine in the brain may have
an effect on ejaculation, and this knowledge has led to some of the
treatments that are currently utilized for ejaculatory problems in men.
Male sexual dysfunction
Male
sexual dysfunction (MSD) is a disruption of any component of a man’s
sexual response leading to significant frustration or distress on the
part of the man or his sexual partner.
Why is male sexual dysfunction an important problem?
Sexual problems can be detrimental to a man’s mood, sense of self-esteem, and quality of life. There
is evidence to suggest that many female partners of men with sexual
problems have sexual problems of their own and that treatment of sexual
problems in men may improve both partners’ sexual functioning.[3]
In
addition, sexual problems may be one of the first signs of a serious
medical condition, such as diabetes, high blood pressure, depression, or
numerous others.[4] Therefore
detecting sexual problems is important not only as a quality of life
issue, but also as a screen for other potentially serious health
problems.
How are male sexual dysfunctions classified?
William
Masters and Virginia Johnson, pioneers in the study of human sexual
function in the 1960’s, devised a model for “normal” sexual function in
both men and women. According to these researchers, normal sexual response follows an orderly set of steps of increasing sexual arousal. The first phase of this process is sexual excitement, followed by plateau, orgasm, and resolution.[5] Helen
Singer Kaplan, a noted New York psychologist, added an earlier phase
labeled “desire” to correspond to an interest in having a sexual
encounter before actual sexual excitement.[6] Although
this model has been criticized and may not apply to all persons, it
remains a useful means of classifying phases of sexual response and
identifying specific aspects of sexuality with which a man may be having
problems.

Adapted from Masters and Johnson (1966) and Kaplan (1974)
In men, sexual dysfunctions may present as disorders relating to differen phases of the sexual response cycle. It
is important to remember that in order to qualify as a true sexual
dysfunction, disorders in any of the phase of sexual response must be
persistent and/or recurrent such that it significantly interferes with
the enjoyment a man and/or his partner derive from sexual activity.
- Problems with Sexual Desire:
- Hypoactive Sexual Desire (HSD) is the absence or notable decrease in frequency of desire for sex. It is normal for sexual desire to decline as a man grows older, but if the decline is sudden or distressing, HSD may be present.
- The opposite of HSD, Hyperactive Sexual Desire, is rare and represents a problem only when it causes personal and/or partner distress, or leads a man to engage in risky behaviors.
- Although it is relatively rare, some men have a strong phobia or sense of disgust towards sexuality. This is known as Sexual Aversion Disorder.
- Problems with Sexual Arousal/Excitement/Plateau:
- Erectile Dysfunction (ED) is the consistent or recurrent inability of a man to attain and/or maintain a penile erection sufficient for sexual activity. [7]
- Problems with Orgasm:
- “Premature” or “Rapid” Ejaculation (PE) is a persistent or recurrent condition in which ejaculation occurs with minimal sexual stimulation before, on, or shortly after penetration and before the man wishes it.
- “Delayed” or “Retarded” Ejaculation (DE) occurs when ejaculation is absent or greatly delayed despite adequate sexual stimulation.[8]
- Problems with Resolution:
- It is normal for men to have a period of time after ejaculation in which they are not sexually responsive. This is known as the refractory period. The duration of the refractory period varies but tends to become longer as men get older. This is not necessarily a problem although some men may be bothered that they cannot repeat intercourse as soon as they wish.
- In some men, erections may persist after sexual excitement has passed. In some cases this leads to a condition called priapism, defined as an erection that lasts an abnormally long time and may lead to serious problems. Priapism is discussed in a separate article.
- Problems with Sexual Pain:
- While this is much more common in women, some men may experience pain with sexual intercourse and/or ejaculation. This may be due to a physical or psychological cause. Physical causes are rare but may stem from abnormalities of the penis or the internal tubes of the male reproductive system.
- While this is much more common in women, some men may experience pain with sexual intercourse and/or ejaculation. This may be due to a physical or psychological cause. Physical causes are rare but may stem from abnormalities of the penis or the internal tubes of the male reproductive system.
How common are sexual problems in men?
Hypoactive sexual desire
Hypoactive sexual desire has been reported to occur in anywhere from 3-17% of men.[9,10] Erectile Dysfunction
Data from the Massachusetts Male Aging Study suggests that over half of men between the ages of 40 and 70 have some degree of ED.[11]
The percentage of men with ED increases with age.[12] In addition to the normal deterioration of body functions, medical problems associated with increasing age (e.g., diabetes, hypertension, high cholesterol) may also contribute to the higher incidence of ED in older men.

Ejaculatory Dysfunctions
Premature ejaculation (PE) is often thought of as a young man’s problem. This stems in part from the common experience of many young men that they ejaculate very rapidly, particularly with a new partner. Despite this perception, epidemiological studies have suggested that concern about “climaxing too early” is an issue for up to 30% of men between the ages of 18 and 60 in the United States, with no real change in prevalence between age groups.[9] Other investigators, however, have found much lower rates of PE.[10] Existing evidence suggests that the rate of PE is relatively consistent around the world, although differences in cultural norms and sexual expectations may cause the reported incidence of PE to vary significantly across countries and cultures.[13]
While patient/partner distress and a man’s sense of control are the most important determinants of whether or not PE is present, PE is more likely to be present in a man who ejaculates within the first minute or two after penetration than a man who ejaculates later. This “rule of thumb” is based in part on a large survey of almost 500 men from Western countries that reported a wide range of intercourse duration among couples. The mean duration of intercourse in this sample was 5.3 minutes. The 2.5% of men who ejaculated the fastest in this group ejaculated in less than 1.3 minutes.[13] The selection of the lowest 2.5% of a group (two standard deviations from the mean) as a cut-off point is a fairly standard scientific method for detection of an abnormality. Accordingly, some clinicians advocate this duration of intercourse as highly suggestive of PE.
Retarded ejaculation appears to be a rarer problem than PE, occurring in roughly 3% of men.[6]
The following conditions have been associated with ED.
Data from the Massachusetts Male Aging Study suggests that over half of men between the ages of 40 and 70 have some degree of ED.[11]
The percentage of men with ED increases with age.[12] In addition to the normal deterioration of body functions, medical problems associated with increasing age (e.g., diabetes, hypertension, high cholesterol) may also contribute to the higher incidence of ED in older men.
ADAPTED FROM PRINS 2002
Ejaculatory Dysfunctions
Premature ejaculation (PE) is often thought of as a young man’s problem. This stems in part from the common experience of many young men that they ejaculate very rapidly, particularly with a new partner. Despite this perception, epidemiological studies have suggested that concern about “climaxing too early” is an issue for up to 30% of men between the ages of 18 and 60 in the United States, with no real change in prevalence between age groups.[9] Other investigators, however, have found much lower rates of PE.[10] Existing evidence suggests that the rate of PE is relatively consistent around the world, although differences in cultural norms and sexual expectations may cause the reported incidence of PE to vary significantly across countries and cultures.[13]
While patient/partner distress and a man’s sense of control are the most important determinants of whether or not PE is present, PE is more likely to be present in a man who ejaculates within the first minute or two after penetration than a man who ejaculates later. This “rule of thumb” is based in part on a large survey of almost 500 men from Western countries that reported a wide range of intercourse duration among couples. The mean duration of intercourse in this sample was 5.3 minutes. The 2.5% of men who ejaculated the fastest in this group ejaculated in less than 1.3 minutes.[13] The selection of the lowest 2.5% of a group (two standard deviations from the mean) as a cut-off point is a fairly standard scientific method for detection of an abnormality. Accordingly, some clinicians advocate this duration of intercourse as highly suggestive of PE.
Retarded ejaculation appears to be a rarer problem than PE, occurring in roughly 3% of men.[6]
What causes sexual problems in men?
What causes Erectile Dysfunction?
ED may result from abnormalities of the nerves that regulate the process (neurogenic ED), reduction of blood flow in arteries (arteriogenic ED), and/or reduced “tightness” of the occlusive mechanism that traps blood in the penis (venogenic ED). In addition, hormonal problems (with testosterone, prolactin and/or thyroid hormone) and psychological issues (depression, stress, anxiety, marital discord, etc.) may also affect erectile function (resulting in hormonal and psychogenic ED, respectively).[1]The following conditions have been associated with ED.
- Coronary artery Disease or Peripheral Vascular Disease (atherosclerosis)
- High Blood Pressure
- Diabetes
- Tobacco use
- Alcohol
- Pelvic surgery that might lead to erectile nerve injury
- Abnormalities of lower urinary tract function
- Depression and/or anxiety
- Pelvic trauma
- Neurological diseases such as Parkinson’s or multiple sclerosis
- Obesity
- Sleep apnea
- Low testosterone
- Low physical activity
- Prescription drugs, including drugs taken for high blood pressure, depression, and anxiety
- Illicit drugs such as cocaine, amphetamines (speed), opiates, barbiturates, and marijuana.[1]
Occasional
episodes of ejaculation occurring shortly after penetration are not
necessarily indicative of a problem, particularly during a man’s first
sexual experiences and when he is with a new partner. If the problem is recurrent and distressing, an ejaculatory disorder may be present.
Stress and/or anxiety may be the root cause of PE in many instances and may contribute to an underlying physiological problem in many other cases. Masters and Johnson speculated that men who felt guilty or feared discovery/interruption during their early sexual experiences might become conditioned (or trained) to ejaculate rapidly.[3] Some researchers have suggested that hypersensitivity of the penis is to blame for PE. Others have hypothesized that some men’s brains may be biologically “programmed” by genetic mechanisms to ejaculate at a lower threshold value compared to other men. In other words, there might be natural variation between different men’s brains that modulate how quickly they ejaculate. It is most likely that many factors are at work in the control of ejaculation and no one reason can be conclusively demonstrated as the root cause of PE in a given man.[14]
DE is an even more mysterious disorder than PE. Some investigators have proposed that men who have unrealistic expectations from intercourse with a partner and men who have become conditioned to respond sexually only to masturbation or certain fetishes may account for many cases of DE. Depression or other psychological problems may play a role in DE as well. Interestingly, many medications used to treat depression may also be direct causes of DE. [6]
Abnormalities of thyroid hormone (which is important for regulating metabolism) have been associated with ejaculatory problems. An excess of thyroid hormone has been associated with PE and deficiency of thyroid hormone has been associated with DE.[15]
Before the actual appointment, many sexual health specialists will ask men to complete a short survey of their sexual function. A variety of brief questionnaires for men’s sexual health exist, such as the Sexual Health Inventory for Men (SHIM) and the International Index of Erectile Function (IIEF). Questionnaires of this type may help to screen for certain disorders and may serve as an “ice-breaker” to facilitate open and honest communication between patient and provider.
The most important component of the evaluation by a sexual medicine specialist is a thorough history and focused physical examination. Important points of the history include the nature of the sexual problem, how long it has been present, and any factors that were associated with the onset of the problem. The provider may ask for details of the patient’s most recent sexual encounter; this provides valuable information that will help the provider make an accurate diagnosis.
The physical exam will include a general assessment of cardiovascular and neurological systems as well as general health. Particular attention will be directed towards the genitalia looking for any abnormalities (e.g. small testicles, scarring or loss of feeling in the penis, inflamed prostate, etc.) which might cause sexual problems.
When evaluating a sexual problem, serious consideration should be given to involving or at least communicating with the sexual partner. Some men are hesitant to speak with their partner about these issues, but open and honest communication is essential to maintaining healthy sexual relationships.
In some circumstances, health care providers may recommend a test called nocturnal penile tumescence test using a device called Rigiscan®. This simple test involves placing a soft ring around the penis at bedtime. This ring is connected to a pressure sensor that will record strain on the ring overnight. If the penis becomes hard, the erection will be recorded by the pressure sensor. This test is most commonly used to distinguish between ED that is primarily psychogenic (in which case normal nighttime erections will occur) and ED that has a physical cause (in which case nighttime erections will be reduced or absent).
Additional tests might include pharmacological testing by injecting a drug directly into the penis to stimulate erection. The purpose of this test is to assess the penile blood supply. A useful adjunct to this test is a color duplex ultrasound examination of the penis. This is a very powerful means of assessing the flow of blood in and out of the penis, which may be important in making treatment decisions.
Power Doppler Ultrasound of the Penis
Ultrasound of the penis in the flaccid (soft) state: When the penis is soft, blood flow in the cavernous artery (red in the diagram) is low and the velocity of blood flow (peaks in the lower portion of the diagram) are also low.
Ultrasound of the penis in the erect (hard) state: During penile erection, dilation of arteries causes an increase in blood flow (note the increase in the red area in the diagram) and higher velocity of blood flow (higher peaks in the lower portion of the diagram on the right side)
Psychotherapy and counseling are the principal treatments for cases of MSD due to psychological causes. Psychotherapy and counseling may also be important adjunctive treatments in cases of MSD with a physical cause. The focus of psychotherapy is typically on establishing communications skills between partners and resolving anxiety and sexual confidence issues. Many psychotherapeutic approaches involve educating the man about the physiology of sexual functioning.
Click here to see an animation demonstrating how muscle dilation occurs in the arteries supplying the penis. Animation by Dan Rivera (http://danieljrivera.com)
PDE5I do not enhance sexual desire and should not therefore be considered aphrodisiacs. Moreover, PDE5I will enhance but not initiate erections. Sexual stimulation (kissing, foreplay, penile stimulation, etc.) is required to actually start the process of penile erection.
In the United States 3 PDE5I medications are available for the treatment of ED. They are:
Stress and/or anxiety may be the root cause of PE in many instances and may contribute to an underlying physiological problem in many other cases. Masters and Johnson speculated that men who felt guilty or feared discovery/interruption during their early sexual experiences might become conditioned (or trained) to ejaculate rapidly.[3] Some researchers have suggested that hypersensitivity of the penis is to blame for PE. Others have hypothesized that some men’s brains may be biologically “programmed” by genetic mechanisms to ejaculate at a lower threshold value compared to other men. In other words, there might be natural variation between different men’s brains that modulate how quickly they ejaculate. It is most likely that many factors are at work in the control of ejaculation and no one reason can be conclusively demonstrated as the root cause of PE in a given man.[14]
DE is an even more mysterious disorder than PE. Some investigators have proposed that men who have unrealistic expectations from intercourse with a partner and men who have become conditioned to respond sexually only to masturbation or certain fetishes may account for many cases of DE. Depression or other psychological problems may play a role in DE as well. Interestingly, many medications used to treat depression may also be direct causes of DE. [6]
Abnormalities of thyroid hormone (which is important for regulating metabolism) have been associated with ejaculatory problems. An excess of thyroid hormone has been associated with PE and deficiency of thyroid hormone has been associated with DE.[15]
What causes abnormalities of sexual desire in men?
The most common abnormality associated with low sexual desire in men is deficiency of testosterone, the male sex hormone. As in most other sexual disorders, depression and anxiety may also play a role in HSD.How are sexual problems in men evaluated?
What should a man who is having a sexual problem do?
The first step in evaluating a sexual problem is consulting with a health care provider. A primary care provider can provide an initial assessment and possibly treatment for sexual problems. Some primary care providers may not be comfortable handling complex issues in sexuality and may make a referral to a urologist or other sexual medicine specialist if there is concern for a physical cause of the disorder. Referral to a psychologist or psychiatrist may be helpful if there is no evidence to suggest a physical cause.Before the actual appointment, many sexual health specialists will ask men to complete a short survey of their sexual function. A variety of brief questionnaires for men’s sexual health exist, such as the Sexual Health Inventory for Men (SHIM) and the International Index of Erectile Function (IIEF). Questionnaires of this type may help to screen for certain disorders and may serve as an “ice-breaker” to facilitate open and honest communication between patient and provider.
The most important component of the evaluation by a sexual medicine specialist is a thorough history and focused physical examination. Important points of the history include the nature of the sexual problem, how long it has been present, and any factors that were associated with the onset of the problem. The provider may ask for details of the patient’s most recent sexual encounter; this provides valuable information that will help the provider make an accurate diagnosis.
The physical exam will include a general assessment of cardiovascular and neurological systems as well as general health. Particular attention will be directed towards the genitalia looking for any abnormalities (e.g. small testicles, scarring or loss of feeling in the penis, inflamed prostate, etc.) which might cause sexual problems.
When evaluating a sexual problem, serious consideration should be given to involving or at least communicating with the sexual partner. Some men are hesitant to speak with their partner about these issues, but open and honest communication is essential to maintaining healthy sexual relationships.
What tests are useful to detect sexual problems?
If a man has not had a recent evaluation for potential vascular risk factors such as diabetes or high cholesterol, or if there is concern for other medical issues (such as thyroid problems or low testosterone), several simple blood tests may be taken.In some circumstances, health care providers may recommend a test called nocturnal penile tumescence test using a device called Rigiscan®. This simple test involves placing a soft ring around the penis at bedtime. This ring is connected to a pressure sensor that will record strain on the ring overnight. If the penis becomes hard, the erection will be recorded by the pressure sensor. This test is most commonly used to distinguish between ED that is primarily psychogenic (in which case normal nighttime erections will occur) and ED that has a physical cause (in which case nighttime erections will be reduced or absent).
Additional tests might include pharmacological testing by injecting a drug directly into the penis to stimulate erection. The purpose of this test is to assess the penile blood supply. A useful adjunct to this test is a color duplex ultrasound examination of the penis. This is a very powerful means of assessing the flow of blood in and out of the penis, which may be important in making treatment decisions.
Power Doppler Ultrasound of the Penis
Ultrasound of the penis in the flaccid (soft) state: When the penis is soft, blood flow in the cavernous artery (red in the diagram) is low and the velocity of blood flow (peaks in the lower portion of the diagram) are also low.
Ultrasound of the penis in the erect (hard) state: During penile erection, dilation of arteries causes an increase in blood flow (note the increase in the red area in the diagram) and higher velocity of blood flow (higher peaks in the lower portion of the diagram on the right side)
How are sexual problems in men treated?
What if a medical condition is the cause of sexual problems?
If a health care provider discovers that another medical condition might be the cause of MSD, s/he will direct treatment towards resolving the other condition. If a medication is thought to be the cause, stopping or changing the mediation in question may improve sexual function. Lifestyle changes such as increasing exercise, eating a healthy diet, and quitting smoking have been shown to help improve sexual function.[16] If sexual function does not improve after treatment of other medical problems or medication adjustment, or if no specific cause for MSD can be found, specific treatments for MSD must be considered.What is the role of the partner in treating sexual problems?
Sexual problems are unique in that they affect both the patient and his partner. In some cases, the problem may stem from a misunderstanding of normal sexual function and/or partner miscommunication. The support and involvement of the sexual partner is often an important predictor of whether or not treatment will be successful.What role do psychotherapy and counseling play in the treatment of male sexual problems?
Psychotherapy and counseling are the principal treatments for cases of MSD due to psychological causes. Psychotherapy and counseling may also be important adjunctive treatments in cases of MSD with a physical cause. The focus of psychotherapy is typically on establishing communications skills between partners and resolving anxiety and sexual confidence issues. Many psychotherapeutic approaches involve educating the man about the physiology of sexual functioning.
What medical treatments are available for ED?
The introduction of a highly effective oral treatment for ED in 1998 revolutionized the field of sexual medicine. Phosphodiasterase type 5 inhibitors (PDE5I) work by inhibiting an enzyme (phosphodiesterase type 5) in the penis that breaks down the signaling molecule (cGMP) that causes smooth muscle relaxation in the arteries to the penis. By inhibiting this enzyme, PDE5I leads to an accumulation of cGMP, thus promoting arterial smooth muscle relaxation, increased penile blood flow, and penile erection.Click here to see an animation demonstrating how muscle dilation occurs in the arteries supplying the penis. Animation by Dan Rivera (http://danieljrivera.com)
PDE5I do not enhance sexual desire and should not therefore be considered aphrodisiacs. Moreover, PDE5I will enhance but not initiate erections. Sexual stimulation (kissing, foreplay, penile stimulation, etc.) is required to actually start the process of penile erection.
In the United States 3 PDE5I medications are available for the treatment of ED. They are:
1. Sildenafil (Viagra®)
2. Vardenail (Levitra®)
3. Tadalafil (Cialis®)
All three of these medications have been proven effective in the treatment of ED. There are some subtle differences among these medicines regarding their possible side effects and duration of action. The
common side effects of PDE5I medications are headache, flushing of
face, indigestion, visual disturbance (more common with sildenafil and vardenafil),
and muscle ache (more common with tadalafil). For best results,
sildenafil and vardenafil should be taken on an empty stomach one hour
prior to sexual activity. The drug remains in the body for 4-8 hours and
therefore sexual activity should take place within 4-8 hours of taking
the medication. Tadalafil can be taken with or without food but is
absorbed more slowly and should therefore be taken at least two hours
prior to sexual activity. Tadalafil remains in the body for 24-36 hours and therefore sexual activity may take place within a longer time frame.
All
of the PDE5I currently available in the United States are approved by
the U.S. Food and Drug Administration for "on demand" treatment, meaning
they are to be taken as needed before planned sexual intercourse. In
early 2008, the US FDA approved low dose (2.5 or 5 mg) tadalifil
(Cialis) to be taken as a daily pill for the treatment of ED. The
proposed advantage of this regimen is that it permits greater
spontaniety regarding sexual intercourse. This is an exciting new
treatment regimen for ED but may not be appropriate for all men.
Although
PDE5I medications are very effective, men who are taking nitrate
containing medicines (nitroglycerin, isosorbide, amyl nitrate, and
others) should not take them as this may lead to dangerous drops in
blood pressure. PDE5I medications should also not be taken
within 4 hours of taking alpha-blocker medicines, which are used to
treat high blood pressure and prostate problems. Several
other medicines have been demonstrated to have interactions with PDE5I;
you should review your medicines with your doctor before taking PDE5I or
any new medication. Additionally, PDE5I medications do
not work for all men; estimates on the rate of failure vary but at least
30% of men do not respond to PDE5I treatment.[17]
Will pills designed to treat ED make me go blind?
Several years ago there was a great deal of concern about a possible relationship between PDE5I and a condition called non-arteritic ischemic optic neuropathy (NAION),
a condition which may lead to blindness in one or both eyes. Several
reports of NAION were associated with recent use of PDE5I.
It
is unclear at this time whether or not PDE5I actually increase the risk
of NAION. NAION is known to be associated with many of the same
factors as ED, including age, high cholesterol, age, diabetes,
hypertension, and cigarette smoking so it could well be that men who
developed NAION while using PDE5I would have developed the condition
whether or not they were taking PDE5I. Tens of thousands of men have
used PDE5I without developing this condition, so if future studies do
show an association between PDE5I and NAION the increase in risk is
likely to be very slight.
What other medical treatments are available for the treatment of ED?
Alternative medical treatments are available for men who cannot take or do not respond to PDE5I. Injection
of medications which cause relaxation of arteries and penile spongy
tissues directly into the penis is a very effective treatment for some
men. The most commonly used medications for this purpose include phentolamine, papaverine, and/or prostaglandin E (available commercially as Caverject® and Edex®). This same medication may also be applied in the form of a suppository inserted in the urethra (Medicated urethral system for erection [MUSE®]).
While the thought of putting a needle or suppository into the penis is
frightening for many men, most men who have tried either of these
therapies report that it is either not painful or only mildly
uncomfortable.
What about erections lasting more than 4 hours?
All erection enhancing medicines carry a risk of inducing priapism; this is the condition referred to in most advertising for these drugs as “an erection lasting 4 hours or more.” Prolonged erection leads to oxygen starvation in the penis and can be very painful. Even worse, oxygen starvation may lead to tissue damage that might worsen erectile function. This is a rare side effect of PDE5I treatment but is slightly more common after penile injection therapy. If priapism occurs after taking one of these medications it should be taken seriously and prompt attention from a physician should be sought.What non-medical therapies are available for the treatment of ED?
There are a variety of devices that may help men with erection difficulty. Vacuum erection devices (also known as vacuum tumescense devices) produce a vacuum around the penis which causes blood to rush into the corporal bodies. This blood is then trapped within the corporal bodies using a constrictive band placed at the base of the penis. Surgical implantation of malleable silicone rods or an inflatable penile pump
inside the penis are both effective surgical options for men with ED
who do not respond to medications. The most popular type of inflatable
(hydraulic) penile implant used in the US consists of a saline reservoir
placed inside the pelvis, a control pump inside the scrotum, and two
cylinders in the corpora cavernosa. Pressing the scrotal pump transfers
the saline from the reservoir to the penis to produce an erection.
Pressing the release valve reverses the process. These interventions
have restored the ability to have satisfying sexual intercourse for tens
of thousands of men who had failed all other treatments.
What therapies are available for PE?
A number of medical approaches are available for the treatment of premature ejaculation. It is important to understand that while the medical approaches available for the treatment of PE are generally safe, there are no Food and Drug Administration (FDA) approved treatments for premature ejaculation.
Selective Serotonin Reuptake Inhibitors (SSRIs)
This class of drugs includes familiar drugs like Prozac® (fluoxetine), Zoloft® (sertraline), and Paxil® (paroxetine).
Originally developed for the treatment of depression, these drugs
inhibit the reabsorption of serotonin in the neuronal synapses
(connections between nerves through which they communicate). Because
serotonin stays in the synapse longer during SSRI treatment, the
ejaculatory inhibiting effects of serotonin in the brain are enhanced. [18]
Generally,
daily administration of SSRI for the treatment of PE is more effective
than on demand dosing but some men do not wish to take a daily pill for
PE. Some sexual medicine specialists have suggested a short course of daily treatment followed by on demand use of SSRI.[18]
The use of SSRI for PE is generally safe although nausea, dizziness, headache, and/or other side effects may occur. These
drugs may also cause some sexual side effects such as decreased sex
drive, ED, and even complete absence of ejaculation. Men who are on
daily dose SSRI should not abruptly stop the medication without speaking
to their doctor as this may cause potentially serious mood effects.
Recently, there has been interest in a medication called dapoxetine, a short acting SSRI which is in development specifically for the treatment of PE. Initial
studies of the drug showed promising results in the treatment of PE but
the drug has not been approved by the FDA due to concerns about the
safety of this medication.[19]
Topical Anesthetics
Application of a numbing gel or cream to the penis has been utilized for decades as a means of treating PE. In
theory, lessening (but not completely abolishing) the sensitivity of
the penis will decrease the amount of sexual excitement a man
experiences with penile stimulation. When utilized
properly, this treatment has been shown to significantly prolong the
duration that some men are able to engage in sexual intercourse and to
improve sexual satisfaction.[20]
Possible
side effects of local anesthetics for PE are excessive numbness of the
penis, which might leave a man unable to feel any sexual stimulation; in
this case he might lose his erection or be unable to climax at all. There is also a potential risk that the numbing medication may be absorbed by a man’s sexual partner. This may decrease the partner’s sexual sensitivity and inhibit sexual climax. For
this reason the medication should be applied for a set, short length of
time prior to intercourse and then thoroughly washed off before
penetration.
PDE5I for PE
While
not designed or approved for the treatment of PE, some researchers have
studied the use of PDE5I medications for the treatment of PE. Several
small studies have indicated that these drugs might have some
beneficial effect in the treatment of PE but others have not shown such a
benefit.[21]
PDE5I
may also be useful in the treatment of PE by shortening the refractory
period, making it possible for some men with PE to have a second episode
of sexual intercourse shortly after premature ejaculation. PDE5I medications are also useful in treating ED that is associated with PE. When both disorders are present, ED should be managed first.
Other medical therapies for PE
A number of other drugs (such as alpha blockers usually used for prostate problems and a pain medication called tramadol) have been investigated for their capacity to delay ejaculation in men. While
several of these drugs have shown promise, they can only be considered
investigational at this point and should not be utilized for PE outside
of a research study setting.
What therapies are available for delay ejaculation (DE)?
The
mainstay of therapy for DE at this time is counseling with a focus on
fostering communication between partners and establishing realistic
expectations from intercourse. Retraining a man to respond to his partner may play a role for some men with DE. While
there have been case studies using drug therapy for this condition, at
this time no medication can be authoritatively recommended for a man
presenting with DE.[6]
What therapies are available for HSD?
Testosterone therapy may improve sexual desire and erectile function in some men with low blood testosterone levels.[22] Testosterone
supplements are available as intramuscular injections, gels or patches
applied to the skin, and as a patch applied to the inside of the cheek. Psychological evaluation may also be indicated for men with HSD.
Conclusions
Sexual problems may not be life-threatening but they can cause significant distress and diminish quality of life. Fortunately, many treatments for these problems are currently available. New
research will continue to improve our understanding of sexuality and
improve treatment for men and their partners who are struggling with
sexual problems in the future.
Additional internet resources:
- Sex Health Matters: (http://www.sexhealthmatters.org/v2/)
- UrologyHealth.org: (http://www.urologyhealth.org/adult/index.cfm?cat=11)
- National Institute of Diabetes and Digestive and Kidney Diseaases (NIDDK): (http://kidney.niddk.nih.gov/kudiseases/topics/erectile.asp)
- American Association of Sexuality Educators, Counselors, and Therapists: (http://aasect.org/)
- Society of the Scientific Study of Sexuality: (http://www.sexscience.org/)
Books on sexual function in men:
- Male Body: A Physician's Guide to What Every Man Should Know About His Sexual Health by Abraham Morgenthaler, M.D.
- Sensational Sex in 7 Easy Steps by Ridwan Shabsigh, M.D.
- Men's Sexual Health: Fitness for Satisfying Sex by Barry McCarthy Ph.D. and Michael E. Metz Ph.D.
- Resurrecting Sex: Solving Sexual Problems and Revolutionizing Your Relationship by David Schnarch, Ph.D.
- A Clinician’s Guide to ED Management by Ridwan Shabsigh, M.D. and Tom F. Lue, M.D.
[1] Dean RC, Lue TF. Physiology of penile erection and pathophysiology of erectile dysfunction. Urol Clin North Am. 2005 Nov;32(4):379-95
[2] Motofei IG, Rowland DL. Neurophysiology of the ejaculatory process: developing perspectives. BJU Int. 2005 Dec;96(9):1333-8.
[3] Goldstein I, Fisher WA, Sand M, et al. Women’s
sexual function improves when partners are administered vardenafil for
erectile dysfunction: a prospective, randomized, double-blind, placebo
controlled trial. J Sex Med. 2005 Nov;2(6):819-32
[4] Kupelian V, et al. Erectile dysfunction as a predictor of the metabolic syndrome in aging men: results from the Massachusetts Male Aging Study. J Urol. 2006 Jul;176(1):222-6
[4] Kupelian V, et al. Erectile dysfunction as a predictor of the metabolic syndrome in aging men: results from the Massachusetts Male Aging Study. J Urol. 2006 Jul;176(1):222-6
[5] Masters WH, Johnson VE. Human Sexual Response. Boston, MA: Little, Brown; 1966
[6] Kaplan HS. The New Sex Therapy: Active Treatment of Sexual Dysfunctions. New York: Brunner/Mazel; 1974
[7]
American Psychiatric Association. Diagnostic and statistical manual of
mental disorders. 4th edition, Text Revision DSM-IV-TR. Washington, DC:
American Psychiatric Association; 2000
[8] Perelman MA, Rowland DL. Retarded ejaculation. World J Urol. 2006 Dec;24(6):645-52
[9] Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and preditors. JAMA 1999 Feb 10;281(6):537-44
[10] Simons JS, Carey MP. Prevalence of sexual dysfunctions: results from a decade of research. Arch Sex Behav. 2001 April;30(2):177-219
[10] Simons JS, Carey MP. Prevalence of sexual dysfunctions: results from a decade of research. Arch Sex Behav. 2001 April;30(2):177-219
[11] Feldman HA, Goldstein I, Hatzichristou DG, et al. Impotence and its medical and psychological correlates: results of the Massachuesetts Male Aging Study. J Urol. 1994;151:54-61
[12] Prins J, Blanker MH, Bohnen AM, et al. Prevalence of erectile dysfunction: a systematic review of population based studies. Int J Impot Res. 2002;14:422-32.
[13] Waldinger MD, Quinn P, Dilleen M, et al. A multinational population survey of intravaginal ejaculatory latency time. J Sex Med. 2005;2(4):492-7
[14] Carson C, Gunn K. Premature ejaculation: definition and prevalence. Int J Impot Res. 2006 Sep-Oct;18 Suppl 1:S5-13 [15] Carani C, Isidori AM, Granata A, et al. Muliticenter study on the prevalence of sexual symptoms in male hypo- and hyperthyroid patients. J Clin Endocrinol Metab 2005;90(12):6472-9
[16] Derby CA, Mohr BA, Goldstein I, Feldman HA, Johannes CB, McKinlay JB. Modifiable risk factors and erectile dysfunction: can lifestyle changes modify risk? Urology. 2000 Aug 1;56(2):302-6
[17] McMahon CN, Smith CJ, Shabsigh R. Treating Erectile Dsysfunction when PDE5I fail. BMC. 2006 Mar 11;332:589-592
[18] Waldinger
MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI
antidepressants on ejaculation: a double-blind, randomized, placebo
controlled study with fluoxetine, fluvoaxmine, paroxetine, and
sertraline. J Clin Pharmacol. 1998 Aug;18(4):274-81
[19] Pryor JL, Althof SE, Steidle C. Efficacy
and tolerability of dapoxetine in treatment of premature ejaculation:
an integrated analysis of two double-blind, randomised controlled
trials. Lancet 2006 Sep9;368(9539):929-37
[20]
Busato W, Galindo CC. Topical anaesthetic use for treating premature
ejaculation: a double-blind, randomized, placebo-controlled study. BJU International. 2004 May;93(7):1018-21
[21] Atan A, Basar MM, Tuncel A, et al.
Comparison of efficacy of sildenafil-only, sildenafil plus topical EMLA
cream, and topical EMLA-cream-only in treatment of premature
ejaculation. Urology. 2006 Feb;67(2):388-91
[22]
Seftel AD, Mack RJ, Secrest AR, Smith TM. Restorative increases in
serum testosterone levels are significantly correlated to improvements
in sexual functioning. J Androl. 2004 Nov-Dec;25(6):963-72